thumbnail
Design EngineeringTechnology and Design Trends to Support an Aging PopulationTechnology and Design Trends to Support an Aging Population
Design engineers have several opportunities to craft technology that promotes safe, independent living for seniors.

.png?width=700&auto=webp&quality=80&disable=upscale)



 Closure device.")
.svg?width=300&auto=webp&quality=80&disable=upscale "Medical device software development")






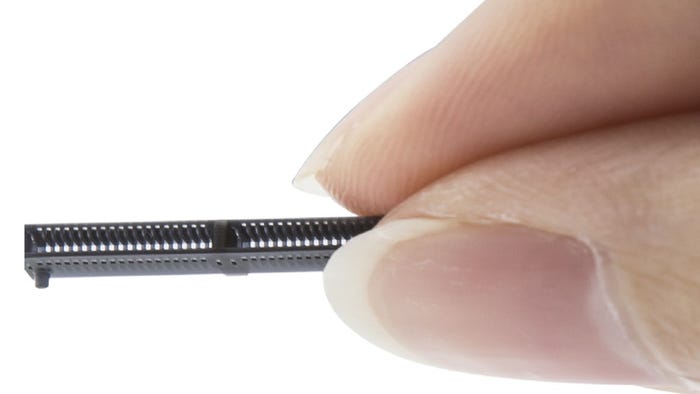
.jpg_(1).png?width=300&auto=webp&quality=80&disable=upscale "MEMS (microelectromechanical systems) pressure sensors in catheter")























Editors' Choice

.jpg?width=300&auto=webp&quality=80&disable=upscale)

Jun 4 - Jun 6, 2024
Jun 4 - Jun 6, 2024
Innovation in automation starts here. Discover and collaborate on automation solutions that are revolutionizing the entire production lifecycle — from design to production to market — and sharpen your competitive edge. ATX South is part of IME South, a six-in-one expo offering the latest insights & solutions spanning medtech, packaging, automation, plastics, design, & processing.
Register NowSign up for the Design News Daily newsletter.